

At least once a week I have a conversation with a young up and coming baseball or softball player about GIRD (Glenohumeral Internal Rotation Deficit). This diagnosis is not just for pitchers; honestly it is really not limited to throwers as we see it in many overhead athletes. So what the heck is it?
GIRD is a change in total range of motion (Arc) comparing the throwing shoulder to the non dominate side. More specifically internal rotation decreases. ROM is usually measured as an arc, approximately 180 degrees with the elbow at shoulder level. When the elbow is pivoted back we call it external rotation and when it goes forward internal rotation. These two measurements should equal roughly 180. (example = ER 130 +IR 50 = 180 degrees of total motion). Many throwers will have a slightly different arc of motion from one shoulder to another, usually the ER on the throwing shoulder is increased and the IR decreased. This shift in motion in and of itself is not pathological, as long as the total ROM of the shoulder remains the same (approx 180). What does cause issues is when the IR is decreased and the change in external rotation cannot compensate causing an overall loss in motion from the usual 180 degrees.
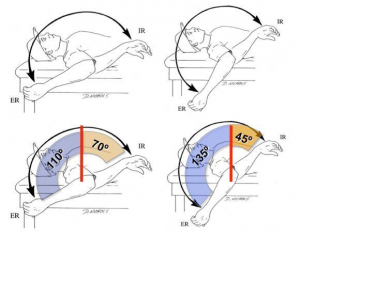 Examples of Arc of motion that can equal 180 and be different from shoulder to shoulder.
Examples of Arc of motion that can equal 180 and be different from shoulder to shoulder.
The shoulder joint is surrounded by joint capsule, or a thick layer of tissue filled with a tiny amount of fluid that lubricates the joint similar to an oiled ball bearing. One of the described causes of GIRD is capsule tightness. The posteriorinferior (back side) of the capsule becomes tight which puts abnormal stress on the humerus bone in the shoulder during motion. This tightness may actually be in response to forces on the opposite side of the shoulder joint (Anteriorsuperior) becoming impinged or squeezed. These anterior structures are the rotator cuff and biceps tendon. Unfortunately over time the increase in posterior tightness places more stress on the anterior structures and a loss of internal rotation can occur along with pain and decreased velocity. This can become a vicious cycle to break.
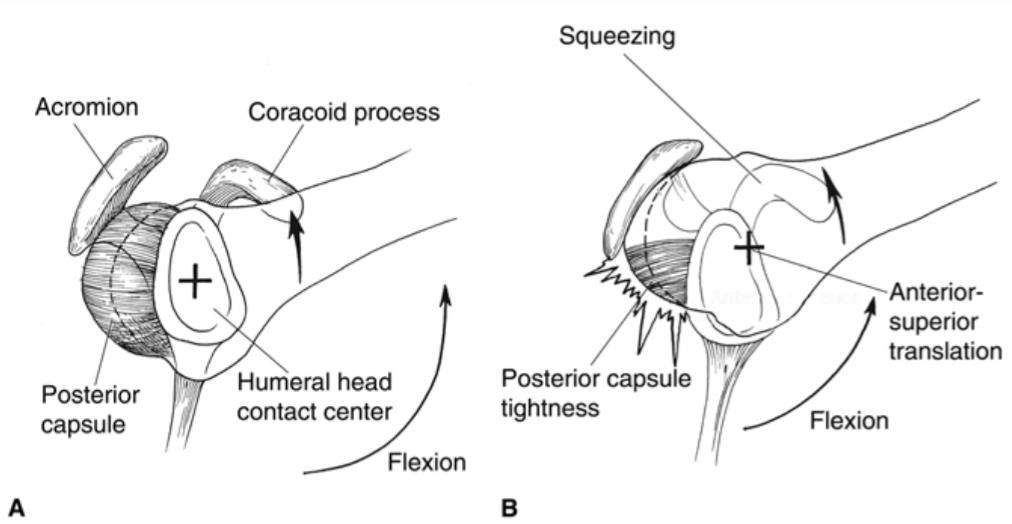 Forces in the back of the shoulder tighten and can change the central pivot point of the shoulder joint. (+ sign here) this shifts the whole joint upward and cause impingement and difficulty with throwing.
Forces in the back of the shoulder tighten and can change the central pivot point of the shoulder joint. (+ sign here) this shifts the whole joint upward and cause impingement and difficulty with throwing.
Fixing true GIRD can involve many steps.
- Resting the affected joint from the overhead sport for a short period of time.
- Anti-inflammatory medication whether it be by mouth or injection.
- Physical therapy by an upper extremity specialist working on capsule stretching and shoulder stabilization.
- Occasionally, we perform MRI scans to rule out other pathology that could be causing pain or lack of range of motion.
- Lastly, a slow interval return to play for the overhead sport.
Rarely does GIRD require surgery but if needed a capsule release can place small slits in the capsule to relieve the tightness in the area. This is only reserved as a last resort and is seen more in postoperative loss of motion.
With persistence GIRD can be eliminated and athletes can return to their given sport to compete. However it is important that they continue the stretching routine to prevent a recurrence over the course of their careers.
 We see GIRD in a variety of overhead athletes including volleyball
We see GIRD in a variety of overhead athletes including volleyball
Sources: